
AUTOR: DR. JOSÉ POLO GARCÍA - MÉDICO DE FAMILIA. CS CASAR DE CÁCERES. CÁCERES
AUTORA: DRA. ELENA RODILLA RODILLA - MÉDICO DE FAMILIA. CS JOSÉ MARVA. MADRID
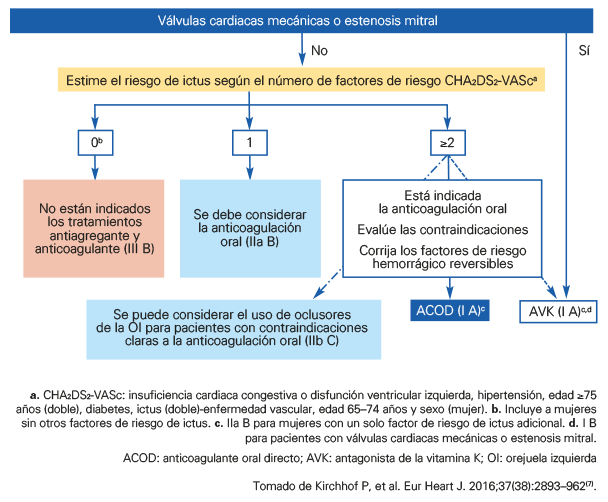
Desde hace años las guías del American College of Cardiology/ American Heart Association/ European Society of Cardiology y de la Sociedad Española de Cardiología recomiendan la anticoagulación oral (ACO) en pacientes con FA no valvular con alto riesgo de complicaciones embólicas y ausencia de contraindicaciones para esta terapia. Sin embargo, aproximadamente 2 de cada 10 pacientes diagnosticados con FA no valvular en España no reciben ACO, siendo el tratamiento en estos pacientes inadecuado18.
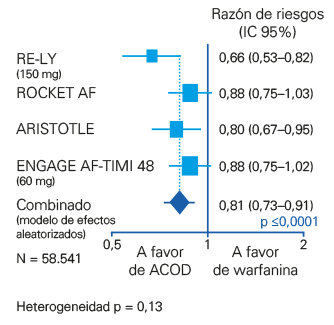
Los ACOD han demostrado en los estudios pivotales y metanálisis no inferioridad, más seguridad y menor número de hemorragias intracraneales (HIC) en comparación con los AVK y las guías los recomiendan sobre los AVK para la gran mayoría de los pacientes con FA no valvular7,8 (FIGURA 12).
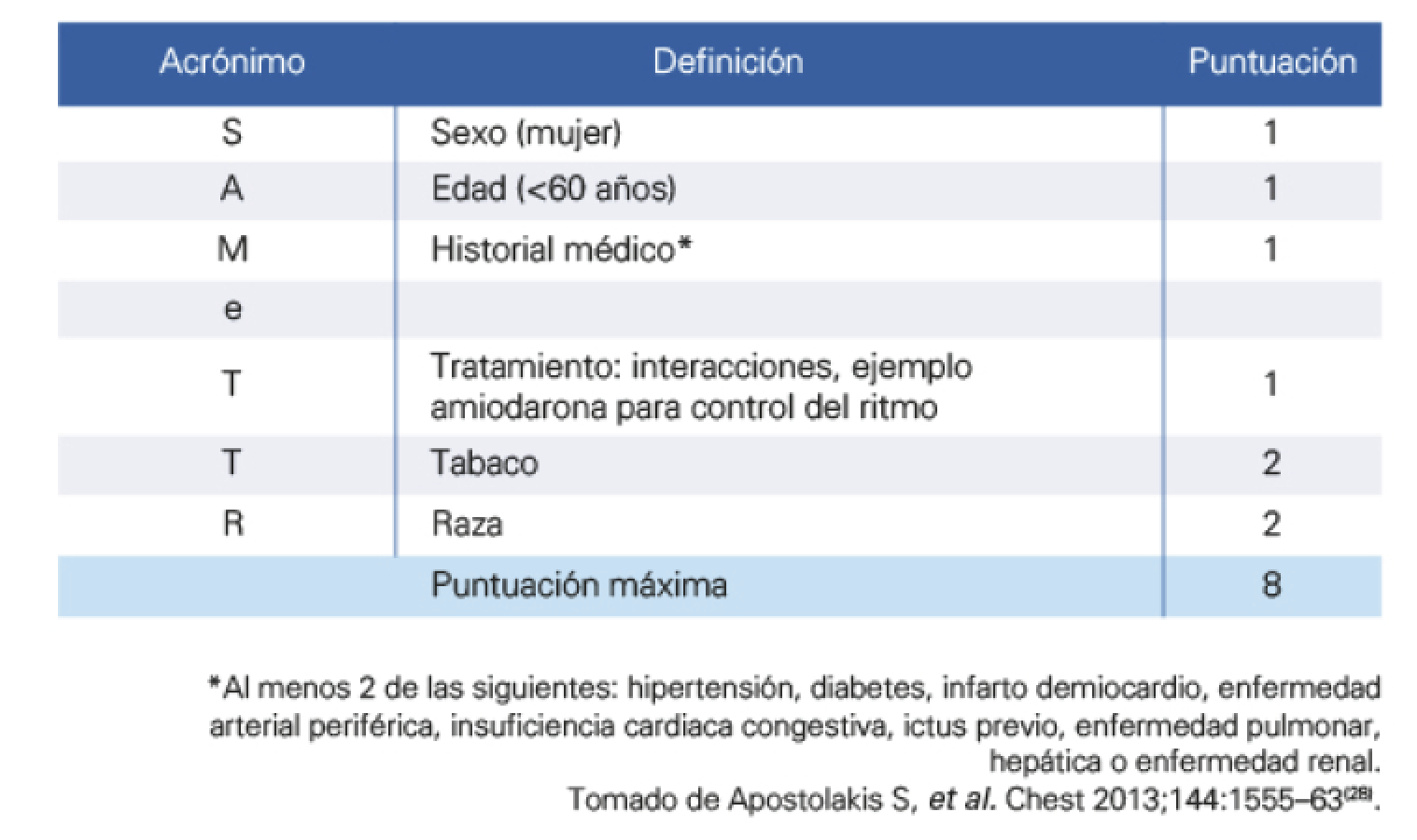
La posibilidad de poder predecir un buen o mal control del tratamiento anticoagulante podría guiar el uso de AVK o de ACOD. Se ha propuesto y validado la escala SAME-TT2R228 (sexo, edad [<60 años], antecedentes médicos [al menos 2 de los siguientes: hipertensión, diabetes, enfermedad coronaria, vasculopatía periférica, insuficiencia cardiaca, ictus previo, enfermedad pulmonar crónica, insuficiencia renal o hepática], tratamiento [fármacos que puedan interferir]; todos estos factores 1 punto; tabaquismo activo 2 puntos, y raza [los no caucásicos 2 puntos]).
La escala SAMe-TT2R2 (TABLA 6) predice qué pacientes presentarán mal control del INR y podría ayudar a la toma de decisiones en el manejo de los pacientes con FA no valvular.
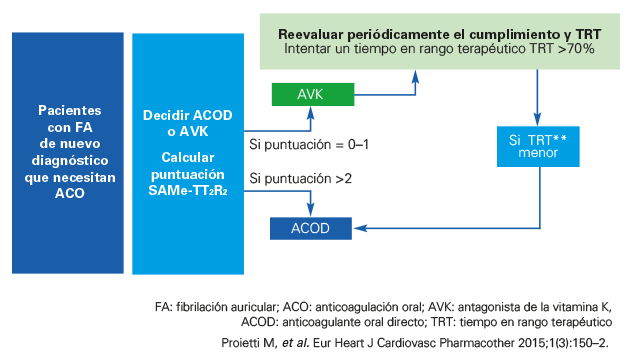
Una puntuación SAM-TT2R2 0–1 indica que los AVK podrían ir bien, y aquellos que presenten puntuación SAM-TT2R2 ≥2 son propensos a tener mal control anticoagulante con AVK y los ACOD podrían ser una mejor opción (FIGURA 13).
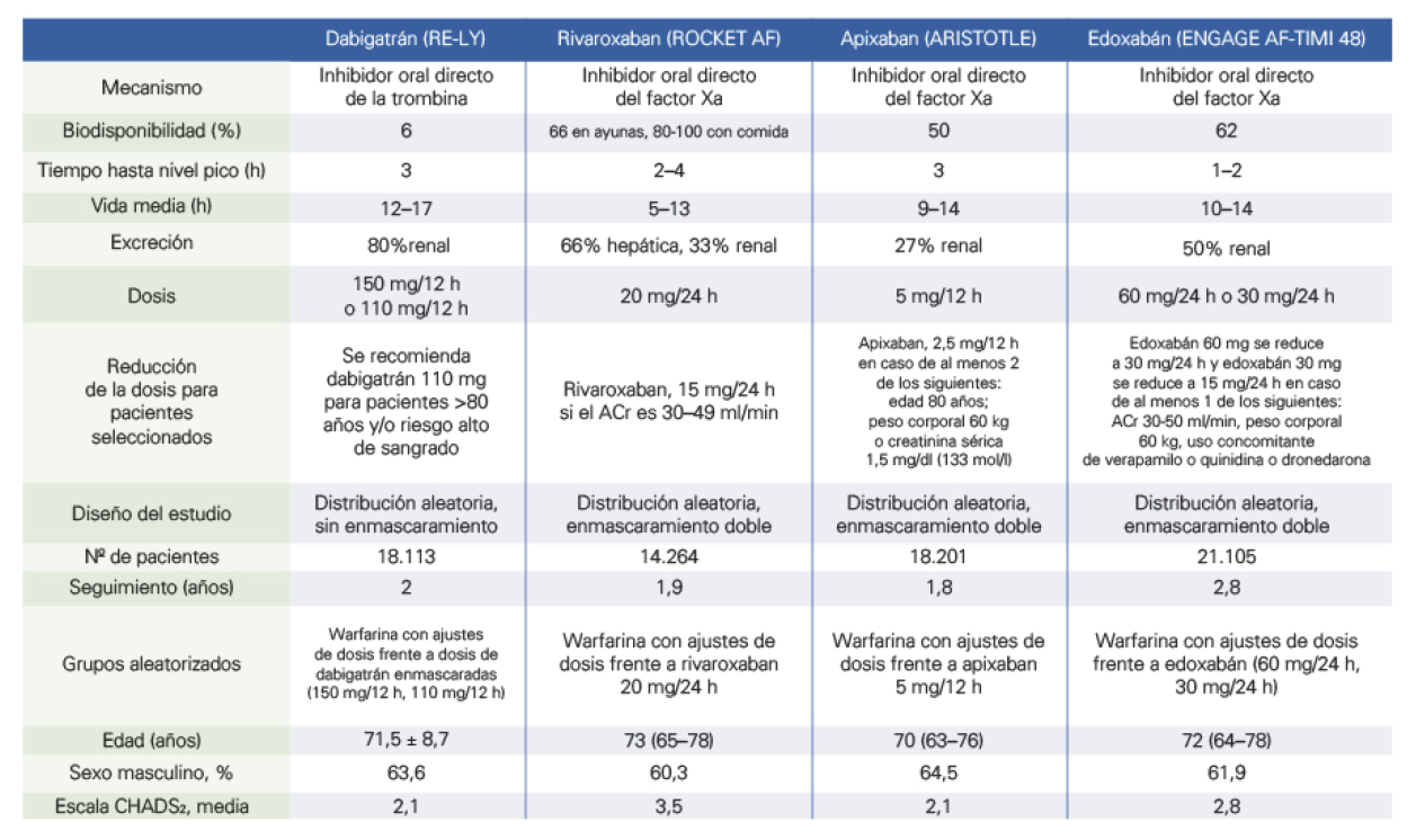
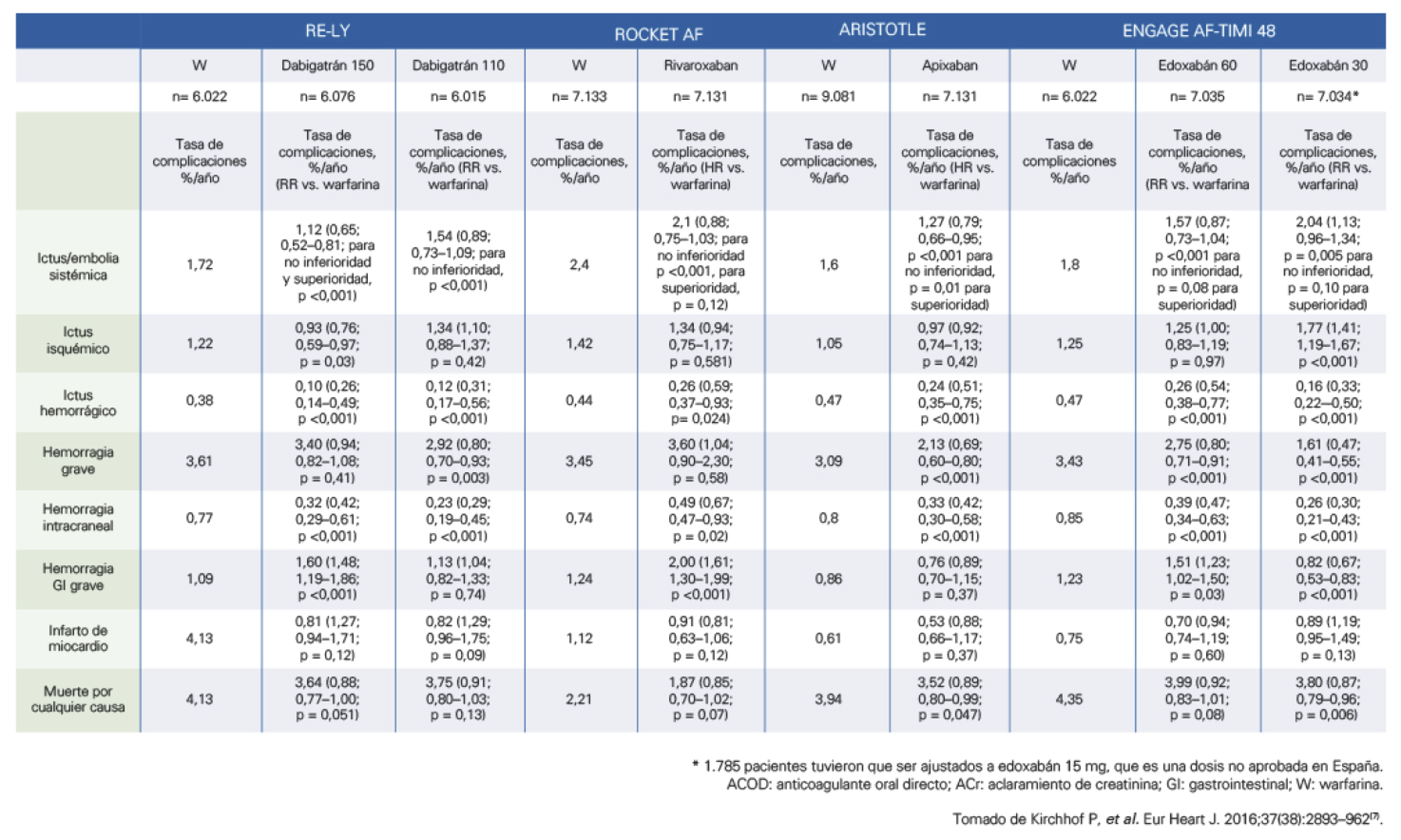
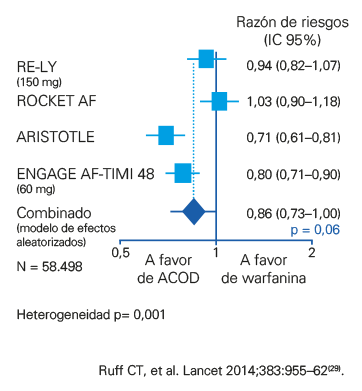
No existen estudios que realicen un análisis comparativo directo de los objetivos de eficacia entre los diferentes ACOD, pero sí podemos obtener algunas conclusiones de los datos obtenidos de los estudios publicados29 (TABLA 7 y FIGURAS 14 y 15).
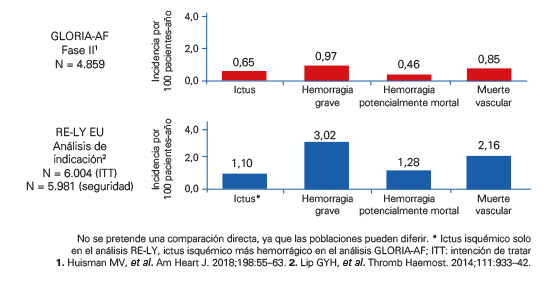
Estudios en vida real30 han ratificado las evidencias de eficacia y seguridad demostradas en los estudios pivotales. El estudio GLORIA-AF31, que incluyó a 2.937 pacientes con un seguimiento de 2 años, puso de manifiesto que el uso de dabigatrán condujo a una baja incidencia de ictus isquémico, sangrado grave e infarto de miocardio (FIGURA 16).
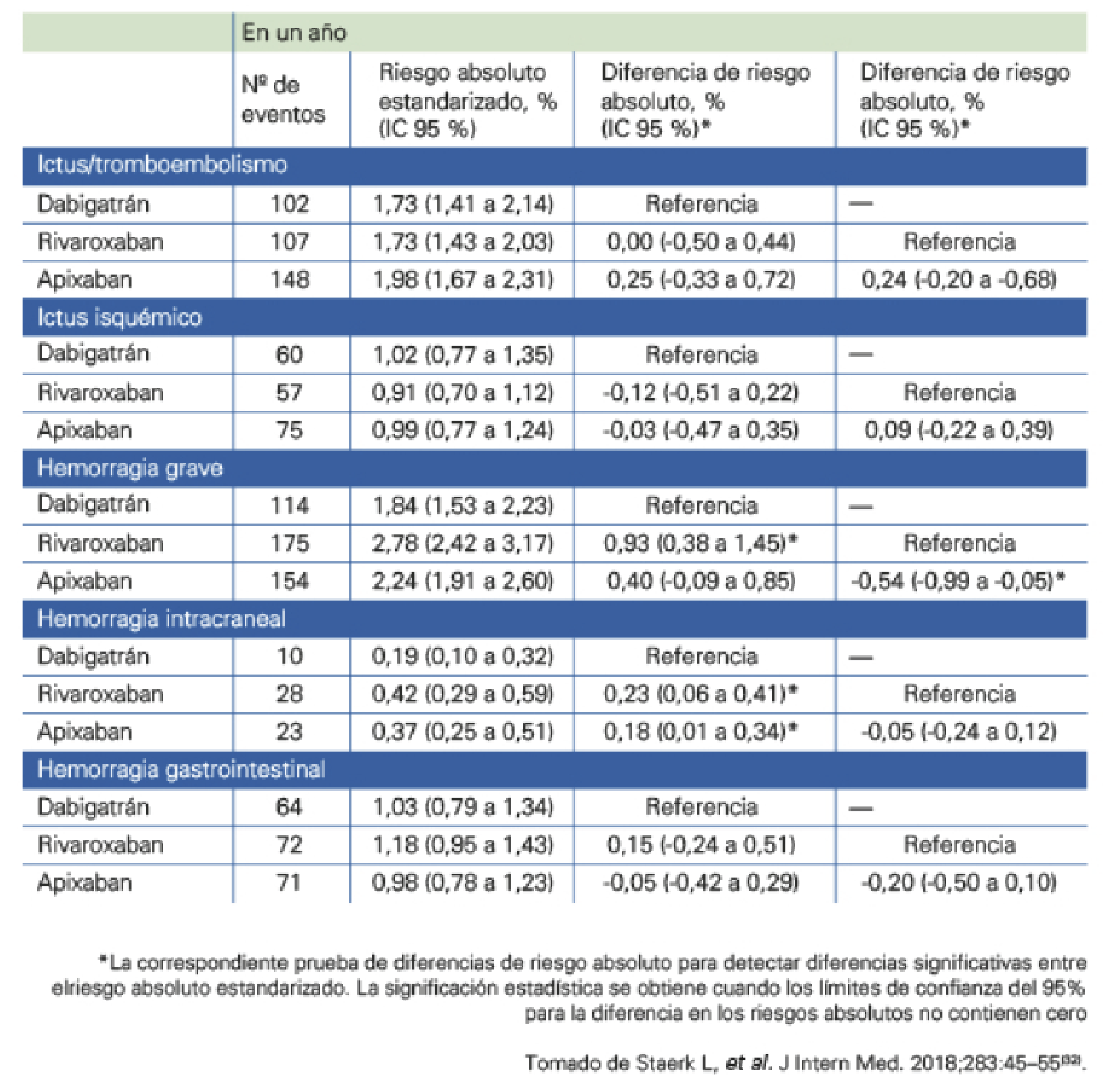
En un trabajo reciente, Staerk et al32 aportan datos de un amplio registro de pacientes daneses tratados con ACOD, y concluyen que dabigatrán se asoció con un menor riesgo de hemorragia intracraneal que rivaroxaban o apixaban (TABLA 8).
En todo paciente anticoagulado es muy importante realizar una prevención de los factores de riesgo que pueden facilitar el sangrado, como son las caídas, el control estricto de la presión arterial, evitar el abuso de alcohol, la polimedicación, la protección gástrica, etc.
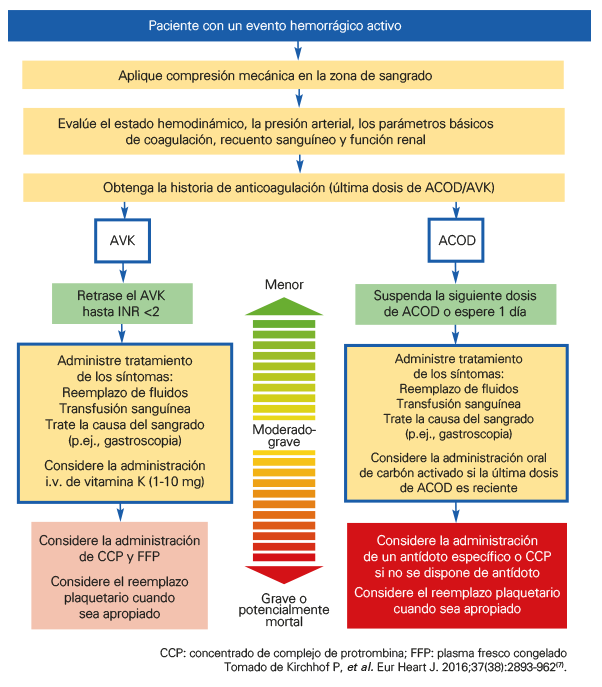
Es obligado en todo paciente con hemorragia realizar una evaluación clínica minuciosa, anamnesis detallada, exploración física, hemograma completo, valorar la función renal y el test de coagulación e INR en pacientes tratados con AVK (FIGURA 17).
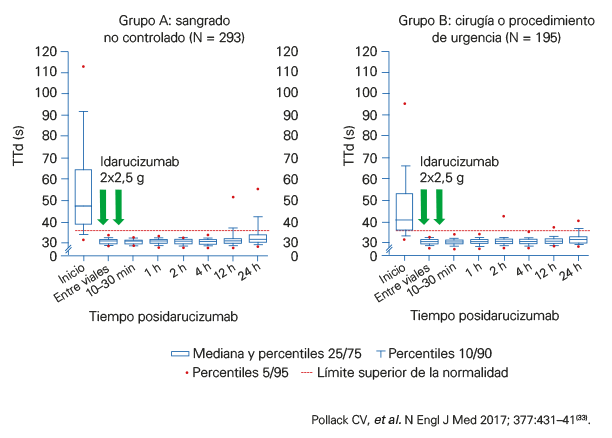
Aunque la terapia con ACOD ha demostrado ser más efectiva y más segura que los AVK, actualmente solo disponemos de antídoto específico (agente de reversión) para los pacientes tratados con dabigatrán. Idarucizumab33 es un fragmento de anticuerpo monoclonal humanizado que se une al dabigatrán y revierte su efecto rápidamente (FIGURA 18).
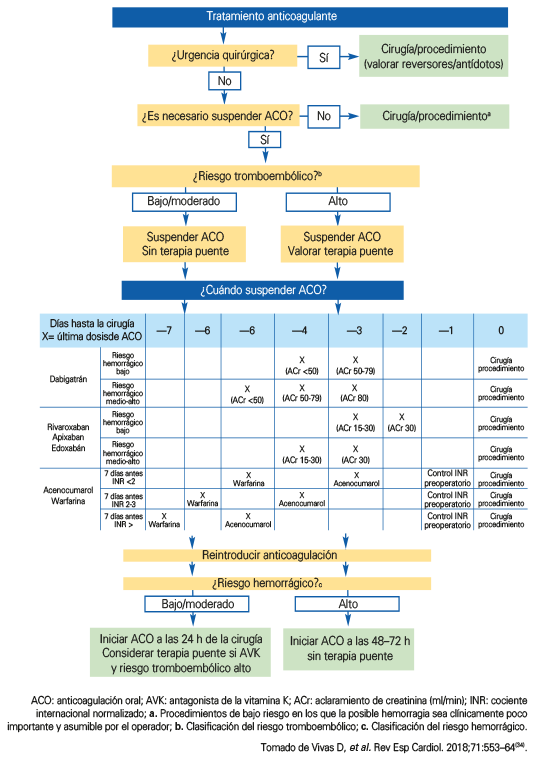
En la mayoría de las intervenciones no sería preciso realizar suspensión del tratamiento anticoagulante. La decisión de retirar o mantener dicho tratamiento estará determinada por el riesgo trombótico y por el riesgo hemorrágico34 (FIGURA 19).
DAB1333.02.2020
